
Treatment Options for Stage 4 Colorectal Cancer Not Responding to Chemotherapy
- Ganesh Akunoori
- Jun 9
- 10 min read


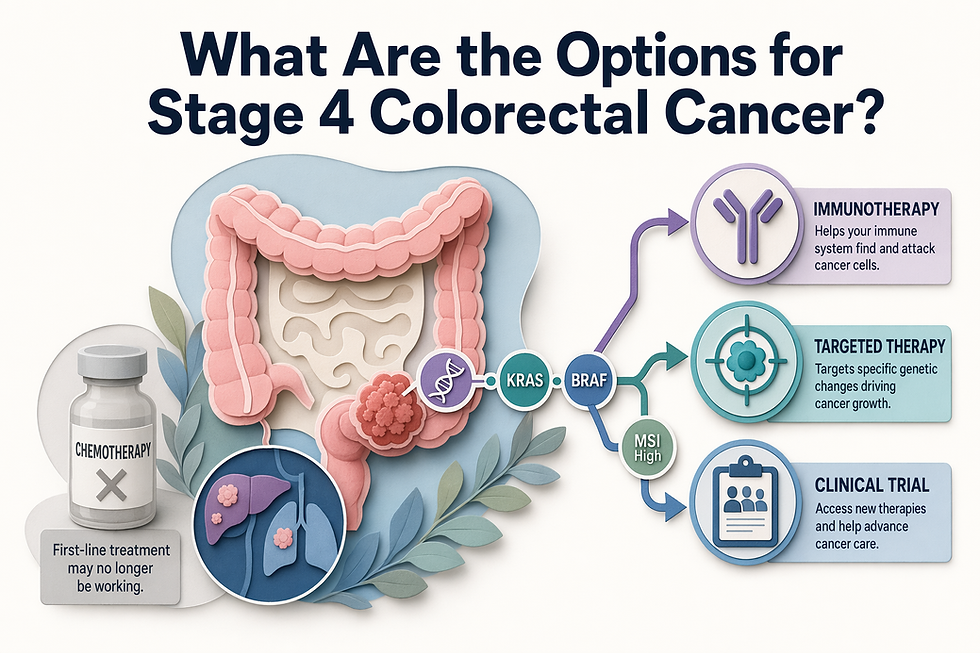
When standard chemotherapy stops working for stage 4 colorectal cancer, treatment eligibility shifts to biomarker-driven therapies targeting specific genetic alterations—not generic late-line drug lists.
Thorough biomarker testing determines access to immunotherapy, targeted therapy combinations, and investigational options based on tumor biology and performance status.
Key Takeaways
Biomarker testing (MSI status, BRAF, HER2, NTRK, KRAS) is the immediate next step after chemotherapy resistance, not another round of cytotoxic drugs
Immunotherapy (pembrolizumab, nivolumab) achieves 40-50% response rates in MSI-H/dMMR tumors but does not benefit the 95% majority with microsatellite-stable disease
BRAF V600E, HER2 amplification, and NTRK fusions unlock targeted therapy regimens with documented clinical benefit in chemotherapy-refractory cases
CAR-T cell therapy for colorectal cancer remains investigational in India, with limited availability and costs ranging from ₹30-50 lakhs
Performance status (ECOG 0-1 vs 2+) determines eligibility for combination regimens versus supportive care pivot
When stage 4 colorectal cancer stops responding to chemotherapy, treatment options shift from cytotoxic drugs to biomarker-driven therapies that target specific genetic alterations in the tumor. Eligibility for these newer approaches—including HER2-targeted therapies, KRAS G12C inhibitors, and immunotherapy—depends on molecular testing and performance status rather than tumor size or prior chemotherapy cycles alone.
Mechanisms of Acquired Resistance in Metastatic Disease
Chemotherapy stops working because cancer cells evolve. Each treatment cycle selects for resistant clones—tumor populations that have acquired DNA repair pathway alterations, drug efflux pumps, or mutations that neutralize the chemotherapy's mechanism. Over successive lines, these resistant clones dominate, and the original regimen loses efficacy. For decades, regorafenib and trifluridine–tipiracil were the only available drugs [1], and both often provided limited clinical benefit compared to best supportive care [1].
The Shift From Cytotoxic to Precision-Based Treatment
The treatment landscape has moved beyond that binary. Several novel systemic treatments have emerged for treatment-refractory metastatic colorectal cancer [1], including trifluridine, tipiracil plus bevacizumab [1] for unselected patients and targeted therapies for subgroups with actionable alterations, HER2-targeted therapies [1] and KRAS G12C inhibitors [1]. The NCCN Guidelines offer multiple treatment options [2] that depend on molecular biomarker testing, and KRAS G12C, targeted therapies are on the horizon [2]. Chemotherapy resistance is no longer the end of systemic therapy, it signals the transition to biomarker-driven sequencing.
Understanding why chemotherapy stops working clarifies the rationale for shifting to molecular testing rather than empiric drug escalation.
Biomarker Testing: the First Step After Chemotherapy Resistance
When first-line chemotherapy for stage 4 colorectal cancer stops working, biomarker testing determines which treatment options remain available. Unlike chemotherapy resistance, which often reflects tumor evolution, biomarker results identify specific molecular alterations that unlock targeted therapies and immunotherapies your tumor may never have been tested for during initial diagnosis. NCCN guidelines recommend thorough biomarker profiling at diagnosis, but many patients only undergo full molecular testing after chemo-resistant progression.

Which Biomarkers Determine Treatment Eligibility
Five biomarkers define your post-chemotherapy treatment pathway:
MSI-H/dMMR status, unlocks pembrolizumab and nivolumab immunotherapy (works in approximately 5% of metastatic colorectal cancer cases with this biomarker).
BRAF V600E mutation, enables combination encorafenib plus cetuximab or panitumumab for anti-EGFR therapy [3].
HER2 amplification, opens access to trastuzumab-based regimens (less common in colorectal cancer but actionable when present).
NTRK gene fusions, qualifies patients for larotrectinib or entrectinib targeted therapy (rare but highly responsive).
RAS mutation status, determines eligibility for cetuximab or panitumumab (only RAS wild-type tumors respond to anti-EGFR agents [3]).
Dr. Bharat Patodiya provides thorough evaluation protocols that integrate biomarker results with multidisciplinary tumor boards, ensuring your care team reviews all actionable findings before recommending next-line therapy.
Testing Turnaround and Treatment Initiation Urgency
Next-generation sequencing (NGS) testing typically requires 2-3 weeks for results. Your oncology team must balance two priorities: starting treatment promptly to control disease progression versus waiting for biomarker results that may reveal more effective options. This is a specialist-led decision without a universal rule, factors include symptom burden, pace of disease progression, and whether archived tissue from prior biopsies can be tested while initiating bridging therapy. When biomarker testing was completed at initial diagnosis, your medical oncologist can access those results immediately to guide post-chemotherapy planning, avoiding the delay.
Once biomarker results return, treatment options stratify by mutation profile, starting with the highest-response subset.
Immunotherapy Options for Msi-H and Dmmr Tumors
Colorectal cancer is the third most commonly diagnosed cancer worldwide[6], yet immunotherapy success hinges on a narrow biomarker gate. MSI-H (high microsatellite instability) and dMMR (mismatch repair deficiency) tumors represent approximately 5% of patients[5] whose cancers accumulate many DNA errors, making them visible to the immune system when checkpoint brakes are released. The other 95% of patients have microsatellite-stable (MSS) disease that does not show a clear benefit from single-agent immunotherapies[5].

Pembrolizumab and Nivolumab: Checkpoint Inhibitors for Msi-H Disease
PD-1 inhibitors like pembrolizumab and nivolumab work by blocking the checkpoint protein that cancer cells exploit to evade immune attack. In MSI-H tumors, high mutation burden produces neoantigens, abnormal proteins that immune cells can recognize once PD-1 brakes are lifted. Response rates reach 40 to 50% in this subset, with many patients achieving durable disease control. Patients considering immunotherapy in India can explore options for immunotherapy access, though biomarker testing is mandatory before initiation.
Who Is NOT Eligible for Immunotherapy
Microsatellite-stable colorectal cancer, the 95% majority, does not benefit from checkpoint inhibition alone[5]. Combination strategies pairing immunotherapy with targeted agents or investigational CAR-T approaches[7] remain under study for MSS disease, but single-agent pembrolizumab or nivolumab will not control disease in the absence of MSI-H or dMMR biomarkers. Patients with liver-predominant metastases should discuss whether regional therapies (ablation, embolization) complement systemic options, as biomarker status alone does not dictate the full treatment sequence.
For the majority without MSI-H tumors, targeted therapy regimens address specific driver mutations identified through thorough genomic profiling.
Targeted Therapy for BRAF, HER2, and NTRK Mutations

When chemotherapy alone cannot control stage 4 colorectal cancer, biomarker testing identifies specific genetic alterations that open access to targeted therapy regimens. Unlike cytotoxic chemotherapy that damages all rapidly dividing cells, targeted drugs block the molecular pathways driving tumor growth in biomarker-positive cases. Three rare but actionable mutations, BRAF V600E, HER2 amplification, and NTRK fusions, each trigger distinct FDA-approved treatment protocols.
BRAF V600E: Doublet and Triplet Targeted Therapy Combinations
BRAF V600E mutations occur in approximately 10% of stage 4 colorectal cancer cases and confer resistance to standard anti-EGFR antibodies. Single-agent BRAF inhibition produces minimal clinical benefit because tumors rapidly activate compensatory EGFR signaling. Combination regimens overcome this adaptive resistance: encorafenib (BRAF inhibitor) plus cetuximab (anti-EGFR antibody) is the FDA-approved doublet, with median overall survival extending to 9.3 months in previously treated patients. For eligible candidates, adding binimetinib (MEK inhibitor) creates a triplet regimen that blocks both BRAF and downstream MAPK pathway reactivation. Your care team coordinates BRAF testing through immunohistochemistry or next-generation sequencing panels before initiating combination therapy.
HER2 Amplification: Trastuzumab-Based Regimens
HER2 amplification appears in 3-5% of chemotherapy-refractory colorectal cancer and activates growth signaling through the HER2 receptor tyrosine kinase. Dual HER2 blockade with trastuzumab plus pertuzumab (both monoclonal antibodies targeting different HER2 epitopes) produces objective responses in approximately 30% of HER2-positive cases. For patients who progress on antibody therapy, tucatinib, a small-molecule tyrosine kinase inhibitor, offers an oral alternative that penetrates the blood-brain barrier, addressing central nervous system metastases. HER2 testing requires fluorescence in situ hybridization (FISH) or immunohistochemistry with reflex FISH confirmation to distinguish amplification from overexpression without gene amplification.
NTRK Fusions: Tumor-Agnostic Larotrectinib and Entrectinib
NTRK gene fusions occur in less than 1% of colorectal cancers but respond dramatically to TRK inhibitors regardless of primary tumor site. Larotrectinib and entrectinib are FDA-approved tumor-agnostic therapies: clinical trials report objective response rates of 75% across all NTRK fusion-positive solid tumors, including colorectal cancer. These oral targeted agents block the aberrant TRK kinase produced by NTRK1, NTRK2, or NTRK3 fusions. Because NTRK fusions are rare, routine testing is recommended only after chemotherapy resistance or through thorough genomic profiling.Dr. Bharat Patodiya coordinates multidisciplinary tumor boards to evaluate biomarker results, confirm FDA approval status versus investigational access, and connect patients with centers offering TRK inhibitor treatment in India.
Key Takeaways
BRAF V600E mutations (10% of stage 4 cases) require doublet or triplet regimens, encorafenib plus cetuximab, optionally adding binimetinib, because single-agent BRAF inhibition fails due to adaptive EGFR reactivation.
HER2 amplification (3-5% of chemo-refractory cases) enables dual antibody blockade with trastuzumab plus pertuzumab or oral tucatinib for antibody-resistant disease and CNS metastases.
NTRK fusions (<1% incidence) achieve 75% objective response rates with tumor-agnostic larotrectinib or entrectinib, but availability in India requires specialist confirmation of FDA-approved import or compassionate-use pathways.
Thorough biomarker testing through next-generation sequencing panels identifies all three alterations simultaneously, avoiding sequential single-gene assays that delay treatment decisions.
When approved targeted therapies and immunotherapy options are exhausted, investigational approaches enter the decision pathway.
Car-T Cell Therapy and Investigational Options in India
Car-T for Colorectal Cancer: Current Investigational Status

CAR-T cell therapy represents a breakthrough immunotherapy approach [8] in which a person's T cells are modified in a laboratory to selectively kill cancer cells [9]. While CAR-T therapies have achieved response rates of 70-83% in blood cancers [8], their application to solid tumors like colorectal cancer faces significant challenges [7]. Colorectal tumors lack universal tumor-specific antigens, and CAR-T cells struggle to effectively infiltrate the tumor immunosuppressive microenvironment [7]. CAR-T cell therapy for colorectal cancer is primarily investigational in India, with limited availability at specialized centers like Tata Memorial Hospital [8]. Most access is limited to clinical trials at specialized centers [8]. Major centers offering CAR-T programs include Amrita Hospital (Kerala and Faridabad), Fortis Hospital (Gurugram), and Manipal Hospital (Bangalore), though most focus on blood cancers [8].
Clinical Trial Enrollment Vs Standard Targeted Therapy: When to Consider Each
Clinical trial enrollment for CAR-T or other investigational therapies typically makes sense after approved targeted therapies (targeting EGFR, BRAF, HER2 mutations) and MSI-H immunotherapy options have been exhausted or when no actionable mutation is found. Dr. Bharat Patodiya provides thorough CAR-T evaluation protocols that include molecular profiling, prior treatment review, and clinical trial screening to help patients understand when investigational access is appropriate versus sequencing standard systemic therapy first. Performance status (ECOG 0-1) and adequate organ function are typically required for trial enrollment, making multidisciplinary tumor boards key for eligibility assessment. Dr.Bharat Patodiya connects patients with leading treatment centers across India for advanced colorectal cancer management.
Insurance Coverage and Cost Considerations for Investigational Therapies
Treatment costs for approved CAR-T therapies in India range from ₹30-50 lakhs [8], though colorectal applications may carry different pricing. Ayushman Bharat coverage for CAR-T is limited, and most patients face substantial out-of-pocket costs for investigational therapies not yet approved for solid tumors. Some clinical trials may cover the investigational therapy cost itself, but patients typically bear associated hospitalization, supportive care, and monitoring expenses. Patient advocates at treatment centers can help coordinate insurance scheme access and assess eligibility for clinical trial enrollment that may reduce direct therapy costs while providing access to cutting-edge investigational options.
Tumor biology alone does not determine treatment access; functional status plays an equally decisive role in eligibility.
Evaluating Treatment Eligibility: What Your Oncology Team Will Assess
When chemotherapy stops working, your eligibility for next-line treatments depends not only on tumor biology but also on your functional status, a factor often missing from online treatment lists.
Performance Status (ECOG Score) and Treatment Tolerability
Your oncology team will assess your ECOG performance status on a 0-4 scale: ECOG 0 means you are fully active and able to carry on all pre-disease activities without restriction; ECOG 1 indicates you are restricted in physically strenuous activity but ambulatory and able to do light work; ECOG 2 means you are ambulatory and capable of all self-care but unable to work, up and about more than 50% of waking hours. Performance status (ECOG 0-1 vs 2+) determines eligibility for aggressive combination regimens vs supportive care pivot. Patients with ECOG 0-1 typically tolerate multi-drug protocols; those with ECOG 2+ often shift to single-agent therapy or supportive care. Dr.Bharat Patodiya's multidisciplinary team integrates performance status assessment into treatment planning, coordinating between medical oncology, surgical specialists, and supportive care to match therapy intensity to your functional capacity.
Liver-Predominant Metastases: When to Consider Liver-Directed Therapies
If your metastases are concentrated in the liver, your team may evaluate hepatic artery infusion chemotherapy (HAIC) or transarterial chemoembolization (TACE) alongside systemic options. Current evidence does not provide a universal algorithm for when to switch from systemic therapy to liver-directed procedures, this decision requires specialist evaluation of tumor burden distribution, liver function, and prior treatment response. Several novel systemic treatments have emerged for treatment-refractory metastatic colorectal cancer, and selecting the most effective later-line therapy remains a challenge, particularly when balancing systemic and regional approaches.
Conclusion
Approved targeted therapies (BRAF, HER2, NTRK regimens) and MSI-H immunotherapy offer evidence-based response rates and should be sequenced before investigational options like CAR-T, which remains limited in availability and insurance coverage in India[1][8]. Performance status (ECOG 0-1) determines eligibility for aggressive combination regimens; patients with ECOG 2+ may benefit more from single-agent options or supportive care pivot rather than pursuing investigational therapies with higher toxicity[10].
The field is shifting from generic late-line chemotherapy fallback (regorafenib, trifluridine, tipiracil) to precision-based sequencing driven by biomarker testing[1], with emerging combination strategies (immunotherapy plus targeted therapy for MSS tumors) and CAR-T engineering advances addressing solid tumor challenges[7].
Get a multidisciplinary evaluation from Dr.Bharat Patodiya to coordinate biomarker testing, second opinions, and treatment pathway planning for chemotherapy-resistant stage 4 colorectal cancer.
Frequently Asked Questions
What is the first step after my stage 4 colorectal cancer stops responding to chemotherapy?
Thorough biomarker testing (MSI status, BRAF/KRAS/NTRK mutations, HER2 amplification) is the immediate next step, not another round of chemotherapy[3][4]. Testing typically takes 2-3 weeks for next-generation sequencing results, and oncology teams coordinate testing with treatment urgency to identify actionable molecular alterations.
Who is eligible for immunotherapy for stage 4 colorectal cancer?
Immunotherapy (pembrolizumab, nivolumab) is highly effective for MSI-H/dMMR tumors, which represent approximately 5% of metastatic colorectal cancers, with 40-50% response rates[5][6]. The 95% majority with microsatellite-stable (MSS) disease does not benefit from checkpoint inhibition alone[5], though combination strategies remain under investigation[7].
What targeted therapy options exist for BRAF V600E mutations?
BRAF V600E mutations occur in approximately 10% of stage 4 colorectal cancer cases and require doublet or triplet targeted therapy, encorafenib plus cetuximab, or triplet with binimetinib, rather than single-agent BRAF inhibition. Single-agent therapy produces minimal benefit because tumors rapidly activate compensatory EGFR signaling pathways.
Is CAR-T cell therapy available for colorectal cancer in India?
CAR-T cell therapy for colorectal cancer is primarily investigational in India, with limited availability at specialized centers like Tata Memorial Hospital[8][9]. Unlike blood cancers (70-83% response rates), CAR-T has not achieved comparable success in colorectal cancer due to the lack of universal tumor-specific antigens[8].
How does performance status affect treatment eligibility?
ECOG performance status (0-1 vs 2+) determines eligibility for combination regimens versus supportive care focus[10][1]. ECOG 0-1 patients can tolerate aggressive combination targeted therapies or immunotherapy, while ECOG 2+ patients may benefit more from single-agent options or palliative care rather than pursuing high-toxicity investigational therapies.
What are the typical costs of investigational therapies like CAR-T in India?
Treatment costs for approved CAR-T therapies in India range from ₹30-50 lakhs[8], though colorectal applications may carry different pricing. Ayushman Bharat coverage for investigational therapies is limited, and most patients face significant out-of-pocket costs. Clinical trial enrollment offers a pathway to access investigational therapies without full commercial cost[8][9].
When should I consider a clinical trial vs approved targeted therapy?
Clinical trial enrollment typically follows exhaustion of approved targeted therapies (BRAF, HER2, NTRK regimens) and MSI-H immunotherapy options[8]. Trials make sense when no actionable mutation is found, approved options are unavailable, or performance status is adequate (ECOG 0-1) for investigational regimens with higher toxicity profiles[9][7].

Comments